Overview
When determining how best to manage hearing loss, it’s important to ensure that the selected approach is likely to provide meaningful benefit for the patient.
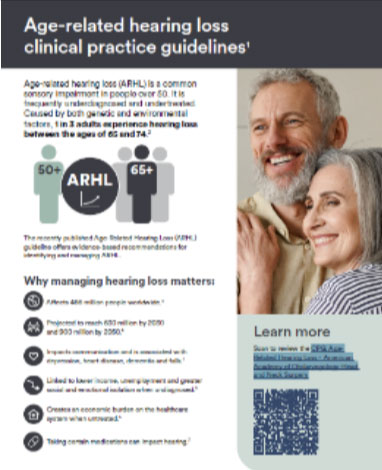
Even mild hearing loss can affect listening and communication. Referral for further audiological assessment is appropriate when screening suggests a possible loss or when a patient or family member expresses concern.

Hear from Drs. Grace and Ryan Casserly, Montage Health on the importance of assessing your patient’s hearing.
Referring for audiological testing
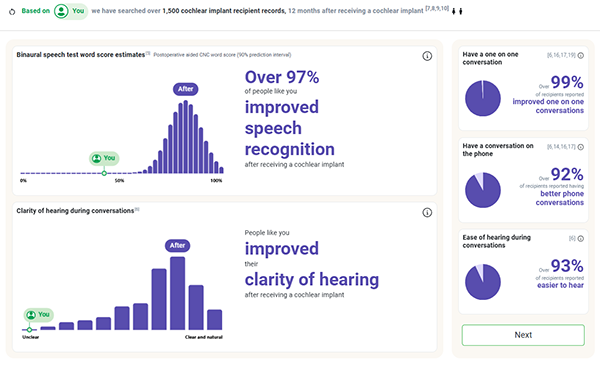
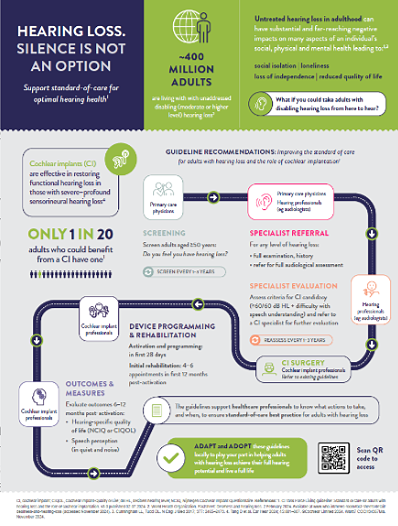
An increasing body of clinical evidence indicates that insufficient management of hearing loss may reduce improvements in hearing function and limit broader health-related quality-of-life benefits associated with hearing rehabilitation.9
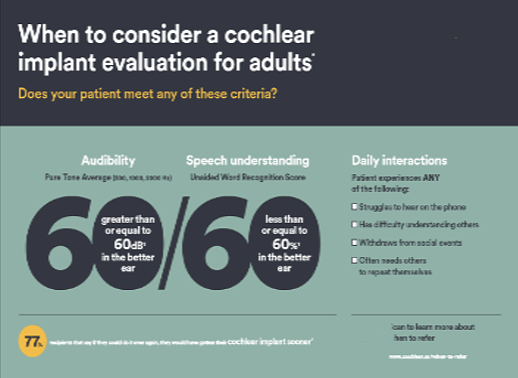
It’s important to refer patients that don’t hear well, even when they are using hearing aids or other hearing solutions for specialist evaluation. Inadequate aiding of a hearing loss results in poor hearing outcomes and puts patients at risk for impacts on their overall health.